This site is intended for Healthcare Professionals only. if you are a member of the general public, click here
ZEPOSIA demonstrated a significant improvement in
clinical remission* at 10 weeks and 52 weeks vs. placebo (primary endpoint)1
You are advised to read the study design information before these efficacy outcomes
Primary endpoint: Clinical remission at week 10 (induction period) and at week 52 (maintenance period)1*

 Pinch & zoom to explore
Pinch & zoom to explore
In the TRUE NORTH study:
- Significantly more patients achieved clinical remission vs. placebo at week 101
- Twice as many patients achieved clinical remission vs. placebo at 52 weeks1
Adapted from Sandborn WJ et al. 2021.
*Patients in cohort 1 were stratified by prior TNFi use and corticosteroid use prior to randomisation.
Please see the True North study design for more information.
†Clinical remission was assessed using the three-component Mayo score and defined as a rectal-bleeding subscore of 0; a stool-frequency subscore of 1 or less, with a decrease of at least 1 point from baseline; and an endoscopy subscore of 1 or less (all on scales from 0 [none] to 3 [most severe]).
TNFi, tumour necrosis factor inhibitor; UC, ulcerative colitis.
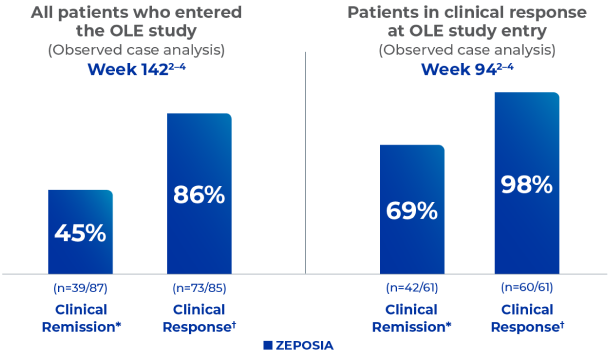
Interim analysis: Long-term clinical response and remission
in the ongoing
TRUE NORTH OLE study2–4
Pinch & zoom to explore
- 116 patients (14%) of those who entered the OLE (N=823) made it to Week 142 of the OLE4
- 276 patients (34%) of those who entered the OLE (N=823) made it to Week 94 of
the OLE4
Data cutoff: September 30, 2020.
*The primary efficacy end point was the percentage of patients with clinical remission at week 10 (for the induction period) and at week 52 (for the maintenance period). Clinical remission was assessed using the three-component Mayo score and defined as a rectal-bleeding subscore of 0; a stool-frequency subscore of 1 or less, with a decrease of at least 1 point from baseline; and an endoscopy subscore of 1 or less (all on scales from 0 [none] to 3 [most severe]).
†Clinical response was defined as a reduction from baseline in the 3-component Mayo score of ≥2 and ≥35%, and a reduction from baseline in the rectal bleeding subscore of ≥1 or an absolute rectal bleeding subscore of ≤1.
References
- Sandborn WJ et al. NEJM 2021; 385(14):1280–1291
- Zeposia (ozanimod) Summary of Product Characteristics, 2022.
- Danese S et al. Long-term use of ozanimod in patients with moderately to severely active ulcerative colitis. Oral presentation at: European Crohn’s and Colitis Organisation (ECCO) Virtual, February 16-19, 2022. Presentation DOP44.
- Wolf DC et al. Long-term use of ozanimod in patients with moderately to severely active ulcerative colitis. Poster presented at: Digestive Disease Week (DDW); San Diego, CA, and Virtual, May 21-24, 2022. Poster Tu1458

Adverse events should be reported. Reporting forms and information can be found at: UK – www.mhra.gov.uk/yellowcard, or search for MHRA Yellow Card in the Google Play or Apple App Store. Ireland-via HPRA Pharmacovigilance at www.hpra.ie Adverse events should also be reported to Bristol-Myers Squibb via medical.information@bms.com or 0800 731 1736 (UK);
© 2022 Bristol-Myers Squibb Company. All rights reserved.
Job: 2084-GB-2300276 Date of Preparation: June 2023